Each April, National Stress Awareness Month is a reminder to recognize the myriad ways stress enters each of our daily lives and to consider its impact on our health. In my work supporting people living with a serious mental illness (SMI) like bipolar I disorder (BD-I), I have observed how increasing stress and disease-related symptoms often go hand in hand.

Clinicians are trained to look for the hallmark signs and symptoms of BD-I–namely, manic or depressive behaviors–which can be identified, in part, through the presence of changes in sleep patterns or energy levels. Stress is often an underlying component of these behavioral shifts, although it is not commonly at the top of the intake questionnaire as something to ask about directly. However, people living with BD-I are not immune to stress; in fact, it’s often quite the opposite. And whether building over time or presenting more acutely, stress on top of BD-I symptoms can impact stability in meaningful ways.
Chronic and Acute Stress
Everybody experiences stress; that’s part of life! But in BD-I, the type and duration of stress can directly and indirectly affect disease presentation and progression.
Chronic stress is a function of day-to-day pressures, whether related to finances, work, relationships, or other forces, that never fully dissipate. Over time, chronic stress can create disruptions in sleep and overall routine. For someone living with BD-I, consistent rest and routine are imperative; as a result, they may feel the effects of stress even more prominently, which in turn can further elevate stress levels.
Acute stress and its impact on mental health is different. In this instance, something significant has happened in the moment, contributing to an immediate and urgent stress response. The concern for people living with BD-I is that acute stress can be highly disruptive and distressing, leading to rapid destabilization and exacerbation of symptoms. Consequently, clinical intervention following acute stress should focus on addressing short-term needs.
Overall, both chronic and acute stress matter. Chronic stress is something providers and patients need to mitigate through long-term management. Acute stress often has to be addressed right away.
Internal Stress Responses
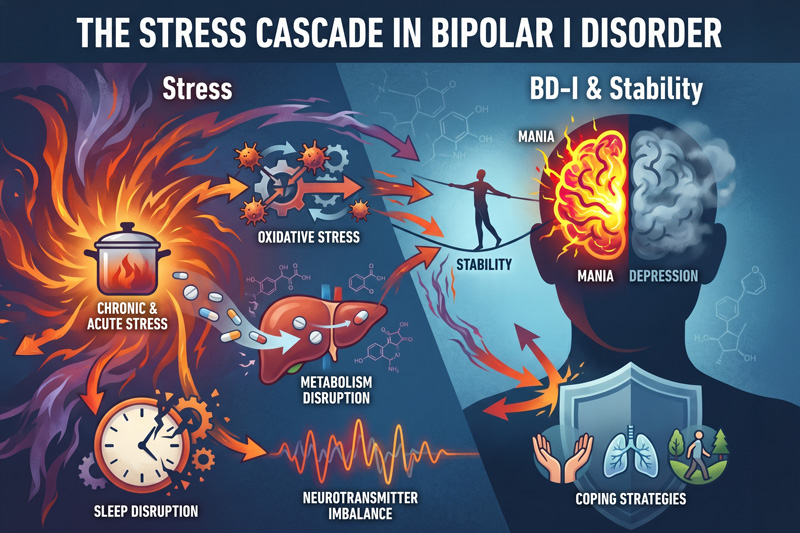
Stress is both a mental and physical reaction, so it has real biological effects. As stress builds in the body, levels of cortisol, a stress hormone, increase. Although cortisol is a natural response to help manage stress, elevated levels for prolonged periods of time can cause a number of processes in the body to dysregulate (1). Ironically, this makes it harder to deal with stress.
Heightened cortisol also can contribute to oxidative stress. Oxidative stress occurs when our bodies’ self-protective systems can no longer keep up with ongoing imbalances, generally driven by external factors, leading to inflammation and cellular damage. For people living with BD-I, an increase in oxidative stress may affect how the body metabolizes medications (2). Potential clinical implications include impact to systems like the liver, which plays a key role in how medications are metabolized. As that balance shifts, the way those medications are broken down can change, along with associated byproducts. This can make it more difficult to maintain consistent, predictable effects from treatment.
Additionally, there are downstream effects on neurotransmitters, such as the dopamine, serotonin and glutamate pathways. When these specific neurotransmitters become destabilized, the brain’s ability to regulate mood is reduced (3). This reflects the cascade effect of stress–it does not occur in isolation, but rather across multiple interconnected systems that are disrupted simultaneously. Eventually, these internal changes result in observable behavioral shifts.
External Signs of Stress
There are often early signs that stress is building to potentially destabilizing levels. For example, changes in emotional regulation are common. Individuals may become more reactive and situations that would otherwise be manageable can feel more overwhelming. For clinicians and loved ones, it’s helpful to be aware that stress responses are not driven by a single moment. Instead, stress compounds over time and eventually something that may seem relatively small creates a disproportionately big response.
Stress also often manifests in sleep disruptions. This is particularly relevant for people living with BD-I because sleep irregularity can be considered both a symptom and an instigator of mania or depression (4).
BD-I is characterized by at least one lifetime episode of mania, featuring symptoms such as increased energy, racing thoughts, talking more than usual, needing less sleep and sometimes more impulsive or risk-taking behavior (5). Sleep is an important factor in accurately recognizing the presence of mania. In fact, sleep disturbances are often one of the earliest signs that a manic episode may be developing and have been cited as the most common prodrome (6). For individuals living with BD-I, even small changes in sleep can increase the likelihood of an episode (7).
The pattern reverses for a person experiencing a depressive episode. During these periods, someone may be sleeping more than usual or they may not be getting restful sleep (4). While the observable result is different, sleep while contending with bipolar-driven depression can still be influenced by stress levels.
In my experience, providers often default to trying to improve patients’ baseline sleep quality, such as through behavioral strategies or medication. This can help. However, if the underlying stressor is not resolved, then the cycle continues, alongside the ancillary effects of adding a medication that may not be necessary if the root cause can be identified and independently managed.
Strategies to Manage Stress
In the moment, there are methods to help regulate the body’s stress response. Breathing exercises are commonly used to calm the sympathetic nervous system. Simple counting or grounding techniques can help redirect focus and reduce an immediate sense of overwhelm. Physical activity is another important component, which provides both a mental and physical outlet to reduce the overall burden of stress.
Access to and awareness of these tools is valuable, but even more important is the ability to identify what activates a person’s stress response in the first place. Once that is better understood, it becomes easier to make adjustments. However, situations will still arise when the stressor cannot be avoided or anticipated. In these scenarios, there is value in recognizing that stress is a natural process and allowing space to step back. Having time to decompress and acknowledge the physical reaction can be part of a long-term approach to maintaining stability.
BD-I is a lifelong condition, and psychosocial interventions complement a thoughtful medication plan (5). We know that excessive stress can impact how well medications work, as well as a person’s ability to take them consistently. Biologically, stress can affect how the body processes medications. Behaviorally, it can disrupt routines, leading to interruptions in treatment adherence. When the goal is managing stress to maintain routines for durable outcomes, both biology and behavior need to be considered.
Stress is not on the sidelines of BD-I care. It’s a central player. Often underlying and sometimes overlooked, stress nonetheless has a major role in how symptoms develop and stability over time. When identified earlier and addressed more directly, there is a better chance of supporting long-term wellbeing.
Dr. Alberto Augsten specializes in expert witness consulting in legal cases, healthcare, and clinical development. A pioneer in healthcare innovation, particularly in psychopharmacology and clinical toxicology, he’s made notable strides in addressing treatment-resistant depression and aiding mothers in recovery. Highly esteemed as a mentor, he actively molds the future of healthcare professionals while extending his proficiency to consulting services, expert witness roles, and advancements in healthcare and clinical practice.
References
(1) Kaur J, Gandhi J, Sharma S. Physiology, Cortisol. [Updated 2025 Dec 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538239/
(2) Banerjee, S., Ghosh, J., & Sil, P. C. (2016). Drug metabolism and oxidative stress: Cellular mechanism and new therapeutic insights. Biochemistry & Analytical Biochemistry, 5, 1000255
(3) Schlaepfer TE, Nemeroff CB. Neurobiology of Psychiatric Disorders. Amsterdam: Elsevier; 2012.
(4) Gold, A. K., & Sylvia, L. G. (2016). The role of sleep in bipolar disorder. Nature and science of sleep, 8, 207–214. https://doi.org/10.2147/NSS.S85754
(5) American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th Ed. Washington, DC: American Psychiatric Publishing; 2013.
(6) Jackson A, Cavanagh J, Scott J. A systematic review of manic and depressive prodromes. J Affect Disord. 2003;74(3):209–217. doi: 10.1016/s0165-0327(02)00266-5.(7) Lewis, K. S., Gordon-Smith, K., Forty, L., & et. al. (2017). Sleep loss as a trigger of mood episodes in bipolar disorder: individual differences based on diagnostic subtype and gender. The British journal of psychiatry : the journal of mental science, 211(3), 169–174. https://doi.org/10.1192/bjp.bp.117.202259
(7) Lewis, K. S., Gordon-Smith, K., Forty, L., & et. al. (2017). Sleep loss as a trigger of mood episodes in bipolar disorder: individual differences based on diagnostic subtype and gender. The British journal of psychiatry : the journal of mental science, 211(3), 169–174. https://doi.org/10.1192/bjp.bp.117.202259